Standard Precautions are guidelines that outline the minimum set of interventions that are required for preventing the transmission of microorganisms. They provide a foundation for infection prevention measures that are to be used for all patients and residents in every healthcare setting. Standard Precautions should be used regardless of an individual’s infection status. All blood and body fluid should be treated as if infectious. Standard Precautions are also referred to as Universal Precautions by OSHA.
Standard precautions include:
-
Hand Hygiene
-
Hand hygiene is the single most effective measure that can be undertaken to decrease the transmission of organisms between healthcare workers, residents, visitors and families. Hand hygiene is defined as cleaning your hands with either soap and water or with alcohol-based hand sanitizer (antiseptic rubs). Alcohol-based hand sanitizer is the most effective product and preferred method to use in healthcare unless hands are visibly soiled or contaminated with spores.
CDC Guidelines for Hand Hygiene >
Hand hygiene must be performed:
- Before touching residents
- Before putting on gloves and PPE
- After touching blood, body fluids, secretions, and excretions
- After touching contaminated items
- Immediately after removing gloves
- Between resident contact
- When moving from a contaminated to a clean body area on the same resident.
Hands need to be cleaned with soap and water:
- When visibly soiled
- When caring for a resident with infectious diarrhea
- After exposures to spores like C. diff
- Before eating
- After using the restroom.
Both the CDC and WHO hand hygiene guidelines are used.
- Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force >
- CDC Clean Hands Count Campaign >
- WHO Guidelines on Hand Hygiene in Health Care >
Other key components:
A comprehensive hand hygiene program should include skin and nail care. Skin irritation by hand hygiene agents is an important barrier to appropriate compliance. Superficial skin layers contain water to keep the skin soft and lipids to prevent dehydration. Hand soaps can increase skin pH, reduce lipid content, increase water loss, and even increase microbial shedding. Soaps are damaging when applied to skin on a regular basis. Alcohol-based hand sanitizers are less irritating than soaps. Using hand lotions and creams are a strategy for preventing infections as heavy hand washing can damage skin, leaving it dry and cracked which can creates a condition for bacterial growth. Hand lotions and creams can prevent skin dryness and keep skin healthy.
Only lotions and creams that are approved by the facility should be used by healthcare workers, as some products:
- Interfere with the hand sanitizers ability to clean
- Are not compatible with CHG (Chlorhexidine gluconate)
- Are not compatible with healthcare gloves
- Can become contaminated with bacteria.
The best way to determine if a product is compatible is to ask the company that supplies the facility with hand hygiene products.
Microorganisms can live under artificial nails, in the cracks of chipped nail polish and in jewelry. Outbreaks of Pseudomonas aeruginosa, extended-spectrum beta-lactamase-producing (ESBL) organisms, Serratia marcescens, and Candida albicans have been linked to healthcare worker’s nails.
Healthcare workers that provide direct care to patients and residents, handle medication, handle supplies, or handle food should not:
- Wear artificial nails, nail enhancements or nail jewelry
- Have natural nails longer than ¼” from the end of the fingertip
- Have nail polish that is chipped or cracked, if worn at all
- Have jewelry, including bracelets and ornate rings on their hands. There is a possibility that these items harbor harmful microorganisms.
More information on outbreaks linked to healthcare workers:
- A Cluster of Hemodialysis-Related Bacteremia Linked to Artificial Fingernails >
- Candida Osteomyelitis and Diskitis after Spinal Surgery: An Outbreak That Implicates Artificial Nail Use >
Hand hygiene monitoring should be done by the healthcare facility to establish compliance rates and help with improving healthcare worker and resident safety. Employee should be given real-time feedback on their hand hygiene practices; this will help to increase compliance. Compliance is recorded as a percentage, the number of observed compliances over the number of observations.
Accessibility and acceptability of hand hygiene supplies is also important to be successful with hand hygiene. Supplies used and placement of supplies should be evaluated annually and as needed.
CDC Standard Precautions: Observation of Hand Hygiene Provision of Supplies >
-
Respiratory Hygiene and Cough Etiquette
-
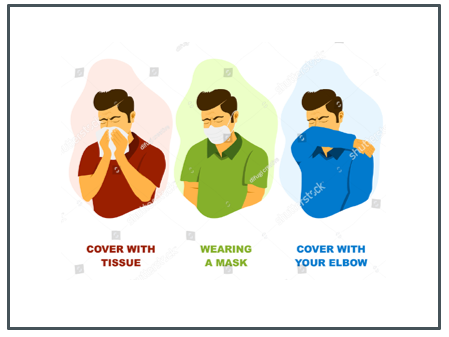
Respiratory hygiene and cough etiquette are the use of control measures to prevent the transmission of respiratory infections, including influenza, among individuals. These control measures are used at the first point of contact with potentially infectious people.
CDC guidelines for respiratory hygiene and cough etiquette >
- Respiratory hygiene and cough etiquette interventions are intended to limit the spread of infectious organisms from persons with potentially undiagnosed respiratory infections
- Healthcare workers with respiratory illnesses should avoid providing direct patient contact
- Mask should be worn by healthcare workers who demonstrate signs and symptoms of respiratory illness but need to provide direct patient contact
- Offer masks to persons who are coughing including residents and visitors
- Institute Droplet Precautions for residents who have signs and symptoms of a respiratory illness
- Use tissues to contain respiratory secretions
- Cover your mouth and nose with a tissue when coughing or sneezing
- If no available tissues, cough or sneeze into the upper sleeve, not hands
- Place used tissues immediately into a non-touch waste receptacle
- Perform hand hygiene after contact with respiratory secretions
- Place tissues, masks and hand sanitizer in conveniently located stations for residents and visitors
- Place signage with instructions for both residents and visitors near respiratory stations
- Offer a mask to residents and visitors with a cough
- Encourage coughing persons to stay six feet away from other people.
Facilities should incorporate strategies to contain respiratory secretions including:
- Providing tissues and no-touch receptacles for disposal
- Providing convenient dispensers of alcohol-based hand rub, skins cream and other hand hygiene supplies.
-
Appropriate use of Personal Protective Equipment (PPE)
-
Personal Protective Equipment (PPE) should be selected based on the nature of the interaction with the resident and potential for exposure.
Gloves
Gloves should be used any time there is anticipation with a resident’s:
- Blood or body fluid
- Mucous membranes
- Non-intact skin.
Gloves:
- Should be worn at the insertion point of any invasive or indwelling device
- Are used to protect both the employee and resident from exposure to potentially infectious agents that are carried on the hands
- Reduce the risk of cross contamination
- Are single-use items and should not be re-used
- Must be changed between resident contact
- Must be removed after contact with blood or body fluids, mucous membranes, or non-intact skin.
- Must be changed when going from dirty to clean areas
- Must be changed when torn or soiled
- Are used to clean equipment or the environment that may have blood or body fluid exposures
- Are removed in a way that prevents hand contamination
When donning, gloves:
- Should cover the wrists and be the correct size
- Are put on last with other PPE
- Donning should occur outside the room if the resident is on Transmission-based Precautions
When doffing, gloves:
- Should occur without touching the inside of the gloves or hands
- Are usually the first item to be removed
- Doffing should occur inside the room
- Hand hygiene is always performed after removing gloves.
Gowns
Gowns should be worn:
- Any time there is anticipation of contact between a staff members clothing and a resident’s non-intact skin
- When a procedure is likely to generate a splash or spray of blood or body fluids
- When handling a container of a residents’ blood or body fluids that are likely to leak, splash or spill.
Gowns are:
- Used to protect clothing
- Usually put on first when combined with other PPE
- Removed at the point of use, if possible
- Removed without touching clothing or the environment
- Regulated by the FDA >Standards for use are provided by the American National Standards Institute (AMII) >
When donning, gowns should:
- Cover the torso, legs to the knees, arms
- Be wrapped around the waist and neck
- Donning should occur outside the room if the resident is on Transmission-based Precautions.
When doffing, gowns should:
- Be pulled away from the body in a gentle manner
- Be folded or rolled into a bundle and discarded
- Donning should occur inside the room.
- Gowns should not be worn between residents or reused.
Face Masks and Eye Protection
Face masks and eye protection should be worn any time there is anticipation of splashes and sprays to the face
- Masks must cover the mouth and nose
- Eye protection should cover the eyes completely
- Glasses and contact lenses are not eye protection
- Are used alone or with other PPE
- Should not be touched when being worn
- Are replaced when torn or damaged
- Are removed promptly after use
- Are removed after gloves and after hand hygiene has been performed
- Are removed from the sides
- Are not worn around the neck or on top of the head
- Are single use disposable items unless extended use is implemented
- Face masks are regulated by the FDA
AMII provides the standards for protection. The levels are:
- Level 1: Ideal for procedures in which there is low risk of fluid exposure (no splashes or sprays expected)
- Level 2: Ideal for procedures in which there is moderate risk of fluid exposure (splashes or sprays can be produced)
- Level 3: Ideal for procedures in which there is high risk of fluid exposure (splashes or sprays will be produced).
Donning:
- Should occur outside the room
- Should fit snuggly to the face.
Doffing:
- Hand hygiene should occur prior to removal
- Should occur outside the room.
N95 respirators:
- N means not oil resistant; 95 means it filters 95% of airborne particles
- Are used when there is anticipation of contact with a resident that has an airborne infectious disease
- Employees must be fit tested
- Employees must have medical clearance to wear
- Should be NIOSH (National Institute for Occupational Safety and Health) approved >
When using PPE, OSHA (Occupational Safety and Health Administration) has regulations to protect employees. Learn more >
CDC guidelines for appropriate personal protective equipment (PPE) use >
CDC examples of how to put on and remove personal protective equipment (PPE) >
-
Ensuring Appropriate Placement of Residents
-
Single rooms are used when there is concern for transmission or exposure of infectious agents of epidemiological significance, some communicable diseases and for outbreak management.
All individuals needing Airborne Precautions will be transferred to a facility that can accommodate this need.
Individuals can be cohorted if they have like illnesses but should not be cohorted if they have different species of the same disease (e.g., do not put an influenza A resident with an influenza B resident).
-
Proper Handling, Cleaning and Disinfecting of Care Equipment, Devices and the Environment
-
Cleaning: Physically removing all dirt and contamination with friction. Cleaning must be done before disinfecting.
Disinfecting: Destroying or inactivating most microorganisms on an inanimate object, but not bacterial spores.
Dwell Time, Contact Time or Kill Time: The duration a surface must remain wet with a disinfectant to work effectively.
IFU: Information for use.
CDC guidelines for cleaning and disinfecting in health care >
General Guidelines:
- All equipment used for resident care shall be kept clean and in proper working condition
- If items cannot be disinfected, they will be dedicated to a single resident or discarded after use
- Single use resident equipment or care items will not be cleaned and reused for another resident
- Single resident equipment or care items reused for the same resident will be cleaned and disinfected after use
- All equipment used for resident care must be cleaned and disinfected before use on another resident
- Commonly shared areas and furniture will be cleaned and disinfected between use and at the end of each day
- Resident care equipment having contact with non-intact skin, mucous membranes, blood or body fluids, secretions or excretions will be single use
- All disinfectant agents and wipes used for resident care equipment within the facility must be approved by the facility
- Disinfectant agents and wipes will be used according to manufacturer’s instructions. This includes assuring that the agent remains in contact with contaminated surfaces for the time specified by the disinfectant agent and wipe manufacturers and not used beyond their expiration date
- Clean equipment is stored in the clean utility room or clean area
- Soiled or dirty equipment is placed in the soiled utility room or area.
Mobile medication carts and treatment carts should be cleaned and disinfected when visibly soiled and routinely.
Pill crushers should be cleaned between resident use and disinfected at the end of the shift.
Stethoscopes, Blood Pressure Cuffs, Blood Pressure Machines, Thermometers, IV Pumps, Feeding Pumps, and Scissors:
- Should be cleaned and disinfected before and after each resident use with a disposable disinfecting wipe
- Should be discarded and exchanged at any time they become grossly soiled, appear worn, Velcro doesn’t stick, or the integrity is compromised
- Should be dedicated equipment for single resident use as required per Transmission-based Precautions
- Should be evaluated prior to removing from the resident’s room to determine if the equipment is reusable or disposable. If reusable or has limited reuse, clean, disinfect and allow to dry according to the manufacturer’s IFU.
Activity and Rehabilitation Equipment:
- Only washable equipment is used for sharing
- Equipment must be disinfected daily and when visibly soiled
- Rinse equipment thoroughly with water to remove disinfectant residue, if appropriate.
Private Equipment or Care Items:
- Should not be shared
- Should be cleaned and disinfected when visibly soiled
- Rinsed thoroughly with water to remove disinfectant residue, if appropriate
- Upon discharge should be discarded or sent home.
CPAP and BIPAP Machines:
- Should remain in the resident’s room when not in use
- Should be cleaned and disinfected weekly and when visibly soiled
- Water reservoirs (if equipped) should be emptied each morning and refilled at night with distilled water. Do not leave water sitting in the machine when not in use. Always empty water reservoir before moving or tilting units
- Clean filters weekly; replace per IFU
- Tubing and face masks should be cleaned daily, as recommended by the manufacturer and as ordered by the prescriber. All apparatus must be cleaned before storing
- After masks and tubing are cleaned and dried, store in plastic bags labeled with resident’s name in closets or cabinets designated for resident personal belongings
- Head gear should be hand-washed and allowed to air dry weekly
- Replace tubing every seven days
- Replace plastic storage bags every week
- When no longer in use by the resident, equipment should be returned to a medical clinic for cleaning and storage.
All disposable respiratory therapy supplies, and equipment must be changed whenever visibly soiled including: nebulizers, nebulizer masks, oxygen masks, nasal cannulas, trach collars, and oxygen bottles.
Shower chairs, lifts, and tubs will be wiped down with a disinfectant wipe then cleaned/disinfected by environmental services per facility policy.
Glucometers should be cleaned and disinfected before and after use.
Environmental Cleaning
The CDC’s guidelines should be followed for environmental cleaning. Environmental cleaning is provided by the Environmental Services Department and nursing, as needed. Any new cleaning agent should be registered with the EPA, evaluated by and approved by infection control. Audits for environmental cleaning compliance including high touch areas and terminal cleaning should be done monthly for compliance.
-
Proper Handling of Textiles and Linen
-
Linen and textiles should be handled in a way that prevents contamination of staff clothing and the environment.
Management of Clean Linen
- All clean linens are stored and transported in carts used exclusively for this purpose or in linen carts that have been decontaminated after being used for soiled laundry
- Clean linens should not come into contact with dirty linen
- Clean linen should be stored in either an enclosed cabinet or covered cart
- Reusable cart covers should be cleaned at least weekly
- Remove and replace cart covers that are broken or cracked
- Staff should perform Hand Hygiene before removing linen
- Linen should be removed without being contaminated
- Clean linen should be carried in a manner that does not touch the employees clothing
- Clean linen should be taken directly to the point of use
- Clean linen cannot be placed on the floor, in common areas, or anywhere in the resident’s room where it can become contaminated
- Any textiles that become soiled during storage or handling must be reprocessed.
Management of Soiled Linen
- All dirty linen will be handled as infectious
- Gloves will be used with all dirty linen that has blood or other potentially infectious materials on it
- Gowns should be used as needed under Standard Precautions
- Handle soiled linen as little as possible
- Do not shake or agitate dirty linen
- Do not place dirty linen directly on the floor, or on any clean surface
- Avoid dirty linen coming in contact with clothing
- Carefully roll up soiled linen to prevent contamination of the air, surfaces, and individuals
- If there is any solid excrement on the linen, such as feces or vomit, it should be scraped off carefully with a flat, firm object and put in a commode or designated toilet before putting linen in a designated dirty container
- Place soiled linen into a clearly labeled, leak-proof container in the resident care area
- Do not transport soiled linen by hand outside the specific resident care area from where it was removed
- Reprocess (i.e., clean and disinfect) the designated container for soiled linen after each use
- If reusable linen bags are used inside the designated container, do not overfill them, tie them securely, and launder after each use
- Soiled linen bags can be laundered with the soiled linen.
-
Safe Injection Practices and Point of Care Testing
-
Health care providers and patients are at preventable risk for infections and adverse events when unsafe injection practices are used.
The World Health Organization defines a safe injection as one that “does not harm the recipient, does not expose the provider to any avoidable risks and does not result in waste that is dangerous for the community.”
The CDC has published the One & Only Campaign that focuses on eliminating unsafe medication injections.
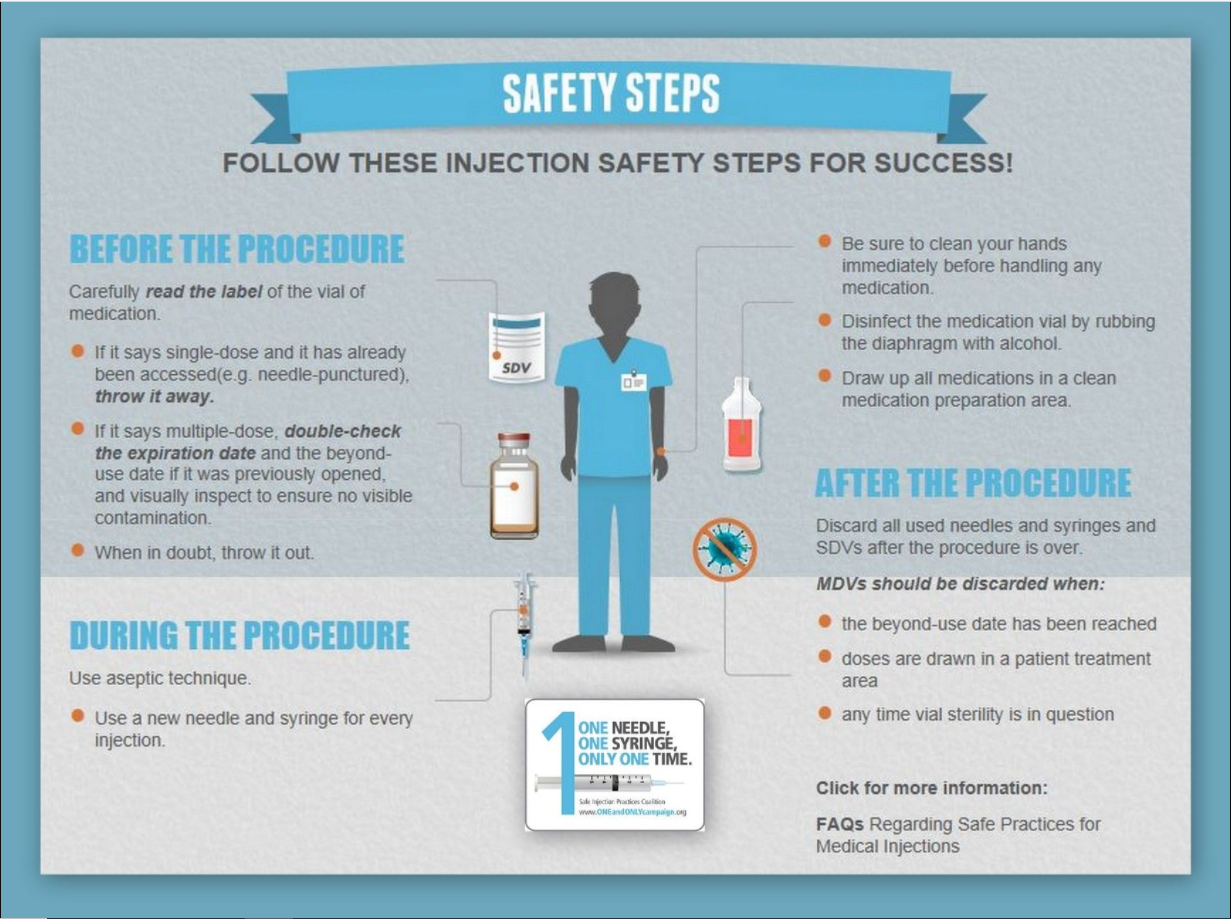
General Guidelines:
- Safety devices should be used for sharps
- Hand hygiene should be performed before and after preparation of medications
- Standard precautions and aseptic technique should be used for preparation and administration of injectable medications and intravenous infusions
- Injectable medications should be prepared in areas that are designated as clean and not adjacent to potentially contaminated areas or water sources
- Disinfect the tops of medication vials with friction for 10 seconds, even if they have a dust cover, with a 70% alcohol prep. Allow the area to dry prior to drawing up medication
- Needles, cannulas and syringes are single-use items. They should never be reused for another resident nor to access a medication or solution that might be used for a subsequent resident
- Do not administer medications from a syringe to multiple patients, even if the needle or cannula on the syringe is changed
- Do not administer medications from single-dose vials or ampules to multiple residents or combine leftover contents for later use
- Do not use bags or bottles of intravenous solution as a common source of supply for multiple residents
- Use single-dose vials for parenteral medications, whenever possible
- If multidose vials must be used, both the needle or cannula and syringe used to access the multidose vial must be new and sterile
- Multidose vials need to be labeled as such to meet the FDA regulations
- Multidose vials need to be labeled and discarded after 28 days. Label the vial with the expiration date
- Do not keep multidose vials in immediate resident care areas
- Store multidose vials in accordance with the manufacturer's recommendations
- Discard multidose vials if sterility is compromised or questionable
- Prefilled syringes, cartridge devices and insulin pens are single resident use only
- Use fluid infusion and administration sets (e.g., intravenous bags, tubing and connectors) for one resident only and dispose after use
- Once it has been used to enter or connect to a resident's intravenous infusion bag or administration set, consider a syringe or needle/cannula contaminated
- Glucose meters should not be shared, if possible. If shared, they should be cleaned between residents with a facility approved disinfectant per manufactures instructions
- Fingerstick devices would never be used for more than one resident
- Sharps should not be bent, broken or damaged in anyway
- Sharps need to be disposed of in a rigid, puncture-resistant container and labeled
- Sharps containers must remain upright, easily accessible and used at the point of care
-
Drug Diversion
-
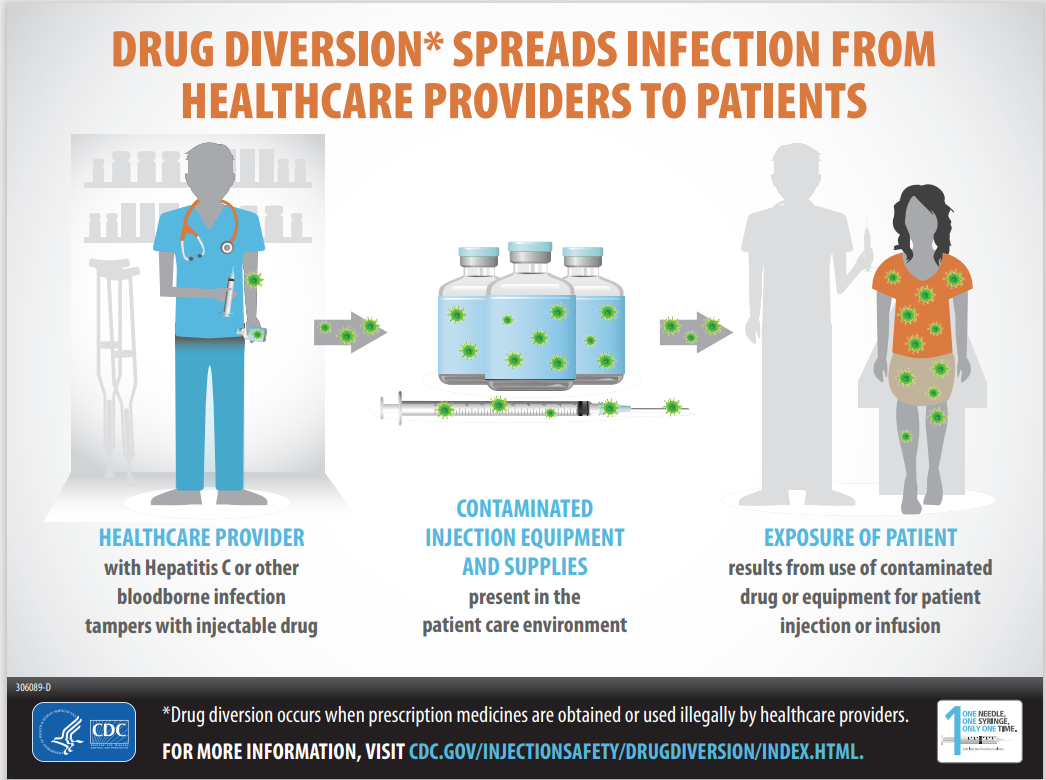
Drug diversion is the transfer of controlled substances from those that were prescribed to another individual for illicit use. When a healthcare provider diverts drugs for their own use it puts the resident at risk for harm including:
- Impaired healthcare workers delivering care
- Denial of pain therapy for the patient or resident
- Risk of infection to the patient or resident if the drug is an injectable.
Outbreaks have occurred during diversion activities to include Hepatitis C and bacteremia. Often when a healthcare worker diverts injectable drugs, they take a syringe that is drawn up for a patient and self-injects the medication then replaces only the needle filling the syringe with saline. The syringe is now contaminated with the user’s blood and given to the patient or resident. It is important to notify a provider if injectable drug diversion is suspected so the resident can be tested and treated for bloodborne pathogen.
Examples
- CDC: Hepatitis C infections associated with a radiology technician at hospitals in New Hampshire, Kansas and Maryland that lead to 45 people becoming infected >
- State of New Hampshire: ver 6,132 patients fulfilled the risk category from this one individual who diverted injectable drugs from 2004 until 2010 >
More Information
-
Ensuring Health Care Workers Handle Needles and Sharps Safely
-
Needlesticks and other sharps injuries are a serious problem resulting in approximately 385,000 injuries to hospital-based healthcare workers each year. Similar injuries occur in other healthcare settings such as nursing homes. Sharps injuries are primarily associated with transmission of hepatitis B virus, hepatitis C virus, and HIV, but they have been implicated in the transmission of other pathogens.
CDC guidelines for ensuring health care workers handle needles and sharps safely >
General Information
- Safe sharps devices should be used whenever commercially available as a substitute for a non-safety engineered device
- The safety device should be engaged before the device is placed into the sharp’s container
- Used needles should not be recapped, purposely bent or broken by hand, removed from disposable syringes or otherwise manipulated
- Used sharps should be placed directly into impervious, rigid, leak-proof and puncture-resistant containers to eliminate the hazard of physical injury. The containers should be appropriately marked with the bio-hazard symbol. Containers should be emptied when they are three-fourths full or are level with the containers line marked “full”.
CDC workbook for designing, implementing, and evaluating a sharps injury prevention program >
Bloodborne Pathogen Exposure Control Plan
Other potentially infectious material (OPIM) means semen, vaginal secretions, cerebrospinal fluid, synovial fluid, pleural fluid, pericardial fluid, peritoneal fluid, amniotic fluid, saliva in dental procedures, anybody fluid that is visibly contaminated with blood.
General Information
- Employees or residents who are exposed to blood or OPIM should first clean the area of exposure
- Soap and water should be used to clean any wounds
- Mucous membranes and eyes should be flushed with water
- Serious injuries requiring suturing, or other physician interventions, should be promptly evaluated.
- Blood and OPIM exposures sustained by residents or employees should be reported to clinical leadership and an immediate supervisor as soon as possible
- Supervisors should fill out an event report
- Individuals should have the site evaluated by a healthcare provider who is trained in bloodborne pathogen exposures
- Employees should be referred to the nearest urgent care or employer contracted facility, if needed
- If the source individual is known or suspected of having a bloodborne pathogen, this information should be conveyed to the healthcare provider following-up on the exposure. The source individual’s name or other identifying information should not be given, only the bloodborne pathogen should be divulged
- The follow-up provider should determine the level of risk to the exposed individual
- The follow-up provider should determine if lab testing is needed from the source or exposed individual
- If further testing is needed from the source individual, the source individual’s physician should be notified of the exposure and should receive the request to order labs drawn for HIV, Hepatitis B and Hepatitis C antibodies
- The source individual should be counseled prior to any testing and should provide written consent.
- The source individuals have a right to refuse testing.
- If the source individual is positive for HIV, Hepatitis B and/or Hepatitis C, after lab testing and this is a new diagnosis the physician should be notified for further counseling. Consent should then be obtained, in writing, from the source individual for testing results to be given to the exposed individual’s provider
- The source individual has the right to refuse result reporting after testing.
- Once consent is obtained from the source individual the exposed provider should be notified of the testing results
- Employees and residents should be encouraged to receive the Hepatitis B vaccinations, if they have not already done so or if they have not finished the series
Residents Exposed to Drug Diversion
- The nurse caring for the resident should promptly notify their immediate supervisor and the resident’s physician if drug diversion of injectable medications is suspected
- The resident should receive an evaluation from a provider as outlined above.
-
Other Things to Consider Include Blood Spill Cleanup, Employee Food and Drink, and Waste Management
-
Blood Spill Clean Up
- Spills of blood or other body fluids should be removed, and the area decontaminated using the facility-approved blood spill kit
- Gloves should be worn during cleaning and decontamination
- The manufacturer’s directions should be followed for use of the product in cleaning and decontaminating spill kits
- Should be cleaned and disinfected with an EPA registered product and have a kill claim against Hepatitis, HIV, and other bloodborne pathogens.
Food and Drink
Staff should designate specific locations where food and drinks with lids are allowed on the units. These pre-approved locations should be separate from areas where lab specimens, contaminated equipment, resident belongings and point of care testing is handled.
Waste Management
Medical waste or biomedical waste is regulated by the state health department. General guidelines include:
- Medical waste needing biohazard disposal must be saturated with blood or other potentially infectious material
- Feces, urine and vomitus are not infectious waste unless they have a large amount of visible blood or have a known infection (e.g., C. diff)
- Most garbage, soiled bed linens, and incontinence products do not have any special handling requirements
- For waste to be capable of causing an infection, all five of these factors must be present:
- Dose (amount of waste that is infected is high)
- Host susceptibility
- Presence of a pathogen
- Virulence of a pathogen
- Portal of entry to the host
- Medical waste products include:
- Liquid waste blood
- Products of blood
- Items saturated or dripping with blood
- Items that were saturated or dripping with blood that are now caked with dried blood (including serum, plasma, and other blood components including their containers)
- Personal protective equipment, including gowns and gloves, should be worn when handling and disposing of medical waste
- A single, leak-resistant biohazard bag should be used for containment of medical waste
- If the biohazard bag becomes contaminated or punctured the bag will require placement into a second biohazard bag
- Infectious waste must be segregated from other solid waste at the point of use, staff present should be knowledgeable about the waste’s origin and its hazard potential
- All bags should be securely closed for disposal
- Puncture-resistant containers (e.g., sharps containers) should be placed at the point of use and out of the resident’s reach. These containers are used for discarding scalpel blades, needles, lancets, razors, disposable scissors etc.
- Syringes without attached needles should be considered infectious waste if it contains an infectious agent, blood or blood products and placed in a sharp’s container
- All infectious waste, biohazard bags and sharps containers should be placed in a secure locked location for pick up.